The Chilling Bowel Twist

According to the English dictionary, the word twist has many meanings; it may mean to turn something, or change, to change the meaning of facts of a statement or distort. It also refers to a dance, the twist, in which people stay in one place and twist their bodies from side to side to music- a dance performed with strenuous gyrations especially of the hips. This reminds me of the song by Chubby Checker, THE TWIST which was popular in the 1960s to which music we used to dance during our schooling days.
Here’s a true story of a patient who struggled for survival. It has nothing to do with the dance, the twist. The patient in this case was not in a fit condition to dance and I am sure, it would not have been in his thoughts at that moment, even if he was a good “twister”. The surgeon writing this story used to twist during his young days, but at that moment what was uppermost in his mind was to save the life of his patient using all the resources at hand.
What is this story?
This story is all about the twisting or turning of a certain organ in a patient’s body which took place spontaneously. This serious condition was neglected for a few days by the patient. He was admitted to my ward in a moribund state struggling for survival. It also highlights the role that I, as the surgeon, had to play together with my team to relieve the suffering and save the life of this patient. This is the bounden duty of all of us in the medical profession.
What Human Organs can Twist?
There are a few organs in the body that can twist. The predominant symptom of a twist of a human organ is PAIN. If neglected, serious consequences can occur. Some organs that can twist are:
- Parts of the gastro-intestinal tract – stomach, small intestine, caecum (the first part of the large bowel) and another part of the large bowel called the Sigmoid Colon, which is situated on the left side. This is the most common organ that can twist!
- Parts of the gastro-intestinal tract – stomach, small intestine, caecum (the first part of the large bowel) and another part of the large bowel called the Sigmoid Colon, which is situated on the left side. This is the most common organ that can twist!

A Twist of the Sigmoid Colon
In medical terms, the twist in the sigmoid colon is referred to as a Volvulus. This means a twist or rotation of the sigmoid colon around its mesenteric attachment in an anticlockwise direction (see figure below). This causes a block to the movement of the contents of the bowel and that loop gets distended with gas – a closed-loop obstruction. The bowel above that too gets distended with gas because of the obstruction caused.
The patient has griping abdominal pain, vomiting and constipation. The abdomen gets bloated as a result of which the patient is in severe distress with accompanying breathlessness on occasions. The movement of the bowel loops (peristalsis) can sometimes be seen on the surface of the belly, like a “wriggling worm”. The danger of this condition lies in the fact that the mesentery may become so tightly twisted that the blood flow to the affected part of the bowel is cut-off. That can lead to the death of blood- starved tissue, gangrene and tearing of the bowel wall – a life-threatening event and a medical emergency. This is a dangerous sequel of Volvulus and hence it can be scary at times. Early detection is of paramount importance. In the majority of cases, surgery is required to untwist the twisted loop and thereby relieve the obstruction and restore the circulation to the affected loop of the bowel. Delay can lead to death from complications.

The “chilling twist”
Nimal was working overseas and had returned to the country. He had been suffering from recurrent bouts of pain in his abdomen with constipation and bloating for about three months. With local remedies and the passage of a bowel motion, his symptoms had been relieved. As a result, he had not taken much notice of the pain and had not taken any medical advice or treatment for his illness. However, before long, his symptoms got worse and unbearable, and he was compelled to enter a hospital for medical care after suffering at home for two days. The pain, which was like a gripe initially, had been getting worse gradually and had become continuous, unrelenting and unbearable. He had also noticed that his abdomen was getting bigger and uncomfortable. He was vomiting profusely and was also constipated. It was at this stage that his relations decided to admit him to a hospital. Nimal was now critically ill and in a state of shock and collapse, gasping for breath. The question asked by his relative who admitted Nimal to the ward was whether his “condition was critical and whether he will survive?” Critical – yes, will he survive?
At the time of admission, Nimal was shouting in pain, gasping for breath with his abdomen tense, tender and bloated like a “football”. He was pale like a sheet, his pulse was very weak and his blood pressure was not recordable. These symptoms pointed towards an abdominal emergency, most likely to be obstruction of his bowel. We were not aware at that stage whether in fact, the bowel had lost its blood supply. Considering his symptoms and signs, that was indeed a possibility. He definitely required rapid resuscitation with intravenous fluids and blood before surgery. An X-ray of his abdomen showed that his large bowel was very much distended with gas showing the typical appearance of a twist of the sigmoid colon – “coffee bean sign” which is the hallmark in a Volvulus.

There are alternate methods of treating Volvulus without surgery, but this was an extreme case and surgery was required urgently. Thus, following resuscitation, he underwent emergency abdominal surgery referred to as a Laparotomy where the abdominal cavity was opened.
EMERGENCY ABDOMINAL SURGERY
What did I find during Surgery?
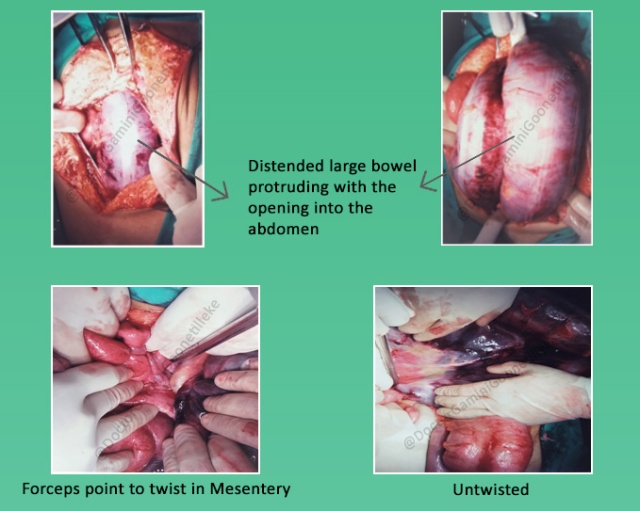
In this operation, the opening into the abdomen had to be done very carefully as the bowel was grossly distended with gas. We were also not sure about the status of the bowel as his symptoms were present for a few days. There was the possibility of the blood supply to that segment of the bowel getting blocked resulting in gangrene of the bowel. Under such situations the bowel can be damaged easily resulting in the contents of the large bowel in this case faecal matter, leaking out and contaminating the entire abdominal cavity leading to a serious infection called Peritonitis which would be fatal.
Opening the abdomen, step by step carefully revealed that the large bowel that was blocked was also ballooned-out and as I displaced that loop I found the “culprit”. That was the loop of the sigmoid colon that had twisted inside the abdomen in an anticlockwise direction. I untwisted this segment very carefully and took it out without damaging the bowel. That loop was black in colour, smelly, dead or gangrenous and in imminent danger of rupture or perforation with the potential leak of faecal contents. That would have been a disaster!

DIAGNOSIS
- Volvulus of the Sigmoid Colon
- Bowel obstruction
- Gangrene of a segment of bowel.
A SCARY SITUATION INDEED!
MORE PROBLEMS AS WE PROCEEDED TO SAVE NIMAL’S LIFE WHICH WAS IN IMMINENT DANGER
Treatment carried out in Stages
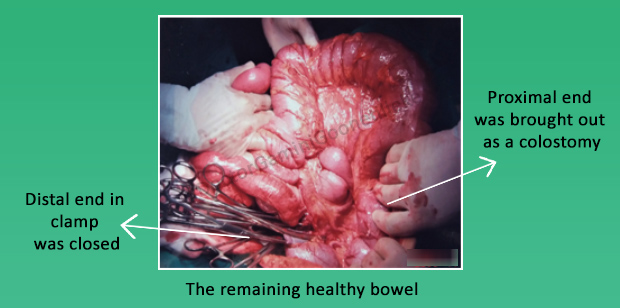
- There was no doubt that the dead segment of the bowel had to be removed. That leaves a gap in the continuity of the large bowel. In non-emergency situations, the two ends of the bowel are brought together with stitches (anastomosis). In this situation, it was dangerous to put the two ends together as the rest of the healthy bowel was swollen and distended with gas because of the obstruction. There was a possibility of the stitches cutting through leading to leakage of bowel contents and more problems.

GOOD JUDGEMENT COMES FROM EXPERIENCE
- In such circumstances, the safest procedure to be done was to close the distal loop and bring the other loop out, referred to as a colostomy. This is an accepted procedure under such situations and is called Hartman’s Procedure.

More Problems
Under normal conditions the opening into the abdominal cavity is closed at the end of the procedure. In this case, we ran into problems. We could not do that!
Why? It was because the bowel that was remaining inside was swollen and had been distended with gas. If I closed the abdomen in the usual manner the abdomen would have been very tense and that could have resulted in further complications.
What’s that? – Closing the abdomen under tension would have resulted in a condition called – Abdominal Compartment Syndrome (ACS) where the pressure within the abdominal cavity exceeds the normal. This would have resulted in further problems for this critically ill patient as it is known that ACS can result in cardiovascular, pulmonary, renal and other complications. This is a well known, but rare problem that a surgeon should be aware of!

No way to leave it open!
It is known that if the abdominal cavity is left open for closure later there is a possibility of drying and desiccation of the bowel. What is usually done under such circumstances is to apply a plastic membrane, what is called a Bogota bag (https://en.wikipedia.org/wiki/Bogota_bag) and stitch it to the edges allowing increased intra-abdominal space and decrease in intra-abdominal pressure. These plastic membranes or Bogota bags were not available to us at that time.
Improvise – We had to look for a substitute, something similar and we found it in an Uri bag (a plastic bag used to collect urine). This was cut according to our requirement and stitched to the edges of the wound with gauze packs underneath.

Intensive Care after Surgery
After the operation, Nimal was managed in the Intensive Care Unit for over a week. Initially, he needed ventilatory support via mechanical ventilation. Antibiotics and drugs to support his blood pressure, cardiovascular and renal systems were also administered. He was closely monitored. His condition improved gradually and was in a fit condition for the next stage in management.
After a week
At this stage, his abdominal pressure had gone down with less tension and was now fit for the suture of the abdominal wound in the usual manner. This was done and he recovered without any further complications.

Recovery
Two weeks later Nimal was in a fit condition to go home, but with a colostomy bag fixed to the colostomy on his abdominal wall with advice on its care. Having a bag hanging outside for a further period of four weeks was a small price to pay for a critically ill patient, now on the way to complete recovery. But he had to wait with that bag till another procedure was carried out four weeks later when bowel continuity was established after another operation, the bag was disposed of and patient had COMPLETE RECOVERY.

“Nimal recovered and now it was time to dance the TWIST to the music of Chubby Checker”

Dear Reader, you might be interested in reading my next blog which was A high-risk adventure to serve the country and the Army : ‘FLYING TO THE NORTHERN WARFRONT IN THE 1990S PART 1’
