The Surgeon’s Dilemma and a Patient’s Worst Nightmare
Background

Extensive injuries to limbs from road accidents, industrial and agricultural accidents are quite common. They can pose serious issues on a victim’s life and the lives of family members with
long periods of hospitalization, economic, psychological, and emotional issues leading to depression and long-term rehabilitation before going back to society to lead an active life. The problems are exacerbated when the amputee is young, with a higher life expectancy and a higher functional demand.
Extensive limb-threatening and life-threatening injuries caused by high velocity bullets and shrapnel of explosive devices occur during a war. Surgical amputation at every level of the lower and upper limbs in victims with critical injuries is a procedure commonly carried out on these victims and dates back to antiquity.
French military surgeon Ambroise Pare (1510 – 90) pioneered modern battlefield wound treatment. His two contributions to battlefield medicine are the use of dressings to treat wounds and the use of arterial ligature to stop bleeding during amputation.
Sudden Loss of a Limb- a Catastrophe
The sudden and unexpected loss of a limb is a catastrophe. During my surgical career, I have seen such incidents and called upon to treat many such victims. The injuries were from road accidents, agricultural and industrial machines, etc. Similar injuries occur in a battlefront from bullets, bombs and mines. Most victims that I encountered were in the prime of their youth and the sudden irreversible act was emotionally devastating for the victims, their families, and for me as well.
On many occasions, the victims pleaded with me not to “cut off” their seriously injured limb even though it could not be saved. These were especially the youth from remote rural villages who had joined the Army to fight the terrorists in the North- East in a long drawn-out battle. They were uneducated and felt that life without a limb was useless. For those who were the bread-winners of the family, the loss of earning capacity and the source of livelihood was badly affected. The reduction in mobility or the loss of mobility in a young man with a long life expectancy was another issue that mattered to the victims.
Variety of Injuries
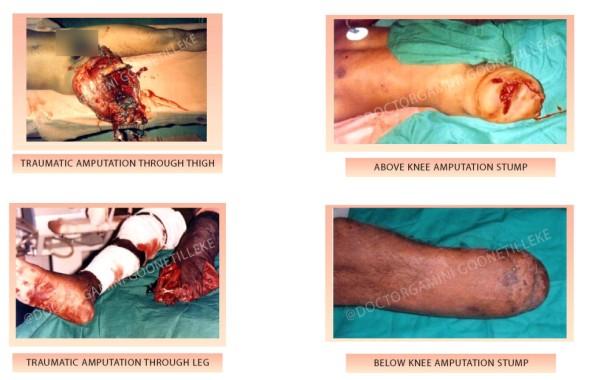
Scenario 1 & 2 – Traumatic amputation or mangled limb
In battlefront hospitals, I have witnessed victims with a variety of injuries. In some, the limb had been blown off (scenario 1) at the time of injury. Then there were others whose limb was “hanging-by-a-thread”, (scenario 2) possibly skin, muscle, or even bone. What is important in such situations is to preserve life as there was nothing I could do except to perform surgery and convert that traumatic amputation in the field to a surgical amputation. This was usually done in stages to make sure that the victim will have a good, healed amputation stump wherever possible that will enable the fitting of an artificial limb so that they can be rehabilitated for gainful employment.
TRAUMATIC AMPUTATION OF LIMB OR SEVERELY MANGLED LIMB
SAVE LIFE
Injuries

Scenario 3 – Extensive injury, but limb can be saved
There were also those with extensive injury to bone and soft tissue, but with no damage to the blood vessels, thus having a good circulation to the limb (scenario 3). There was no risk to life. In these victims, the limbs could be preserved but require surgery, long periods of hospitalisation, and rehabilitation. But the fact is that THE LIMB CAN BE PRESERVED WITH APPROPRIATE MANAGEMENT. THAT IS THE GOOD NEWS FOR THE PATIENT.

Scenario 4 –Surgical dilemma – “Battle on to save life and limb”
Case study

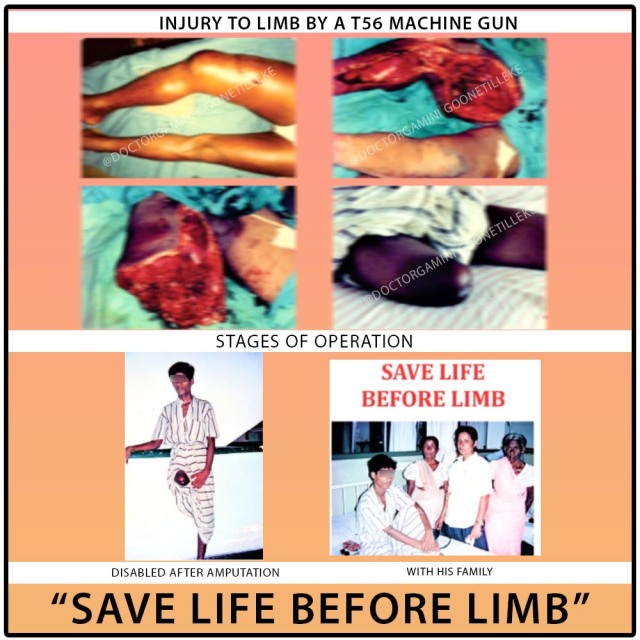
Aruna Shantha was an 18-year-old boy from a remote village in the South of the country. He had joined the Army to fight the war against terrorists when manpower was required to serve in the front line. After six months of intense training, he was sent to the battlefront. Before long, he was injured when he was hit by a bullet from “no-where”. The high-velocity bullet from a T56 machine gun had gone through the upper part of his right thigh. He collapsed on the spot and was rushed to the battlefront hospital. He had no first aid as there were no paramedics to attend to him. On reaching the hospital late in the evening, four hours later, he was in a state of shock and collapsed. This was the only injury on his body.
He was resuscitated with blood transfusion and intravenous fluid and other medications. An X-ray showed that his Femur (thigh bone) was shattered. The limb was tense and swollen with signs that there may be damage to the main blood vessels of his lower limb – the femoral artery and vein. There were no facilities for further investigations. There was no doubt that he required emergency surgery without delay. He was not in a fit condition for transfer to a tertiary care centre with better facilities.
Patient – 18 years
Extreme Swelling of the limb, shattered bone, and no circulation to the limb SURGICAL DECISION – Limb salvage? Amputate through the site of fracture?
Emergency Surgery reveals more about the injury

As the limb was tense and swollen it had to be decompressed by an incision extending from the groin to the ankle. This is called a fasciotomy. This revealed extensive swelling and damage to the muscle caused by the high-velocity bullet in addition to the shattered Femur. It was confirmed that the main artery and vein of the limb were also damaged by the bullet. If the limb was to be saved the main artery and vein had to be repaired and this was given priority. These two vessels were repaired appropriately. This was followed by excision of all the dead and damaged tissues and muscle and the wound was washed thoroughly with normal saline. Gauze dressings were applied to the wound and the fracture was supported by a plaster-slab behind the thigh. At the end of the procedure, there was some oozing as expected because of the large wound, but it was nothing alarming. The patient was taken to the ward for postoperative care as his condition was stable.
WARNING TO STAFF!
With revascularisation and return of blood supply to the limb, especially the muscles, there could be severe bleeding from the wound in view of the extensive damage to muscle leading to shock, collapse and death of the victim. Therefore monitor the condition of the patient carefully and keep me informed.
Torrential Bleeding from the Wound
It was in the early hours of the morning that I was alerted that things were not proceeding smoothly. The patient was bleeding profusely from the extensive injury and had collapsed. His life was on a “cliff hanger” and death was inevitable if the bleeding was not controlled.
ARUNA SHANTHA’S LIFE WAS IN MY HANDS
MY TASK WAS TO CONTROL THE BLEEDING IF HE WAS TO SURVIVE
HE WAS NOT IN A FIT CONDITION FOR ANOTHER MAJOR PROCEDURE
IT IS THEN THAT I REMEMBERED WHAT AMBROISE PARE DID TO CONTROL BLEEDING IN AMPUTATIONS
THE PROCEDURE HE EMPLOYED WAS TO TIE THE ARTERY
I HAD NO OPTION BUT TO TIE THE FEMORAL ARTERY AT THE GROIN.
BLEEDING WAS CONTROLLED
- The battle to save the limb was lost in the early hours of the morning! I retreated to the camp to decide on the next strategy to be implemented later on.
- Now it was a battle to save his life.
- He was not in a fit condition to give consent for this procedure and I had to decide on his interest
- And that decision was to amputate the injured limb at the site of the fracture
- The leg was amputated
- The wound was left open in keeping with the principles of management of war injuries.
Aruna Shantha as expected was a disappointed lad. He had joined the Army to fight for his country, but now disabled for life. What was in store for him in the future? That was the question in his mind!
With time he came to grips with his condition and was happy that his life was saved!
⦁ Once his condition was stabilised he was transferred to the Military Hospital in Colombo. Two weeks later when the swelling had subsided and there was no infection it was possible to suture the wound and he had a stump that could be fitted with an artificial limb.

It was my duty to speak to the relatives of Aruna Shantha, especially his mother, and explain the sequence of events that led to the amputation. They understood the situation. The mother’s position was that my son has lost his leg, but for me, my son is still with us and we will care for him. THAT NO DOUBT IS THE LOVE OF A MOTHER!
Today, Aruna Shantha is one of many disabled soldiers who were injured and lost limbs in the war against terrorism in Sri Lanka. The consolation for them is that they are cared for by the State.

Challenging Situations
Amputation was the treatment of choice for extensive injuries of limbs in the past. The development of modern techniques for limb salvage and team management especially in emergencies (orthopaedic/vascular/plastic), in specialised centres, has produced better results. At the same time there is the surgical, moral, and ethical dilemma which the surgeons face in such situations: limb salvage or amputation/attempt salvage, failing which amputate!
Mangled extremity severity score (MESS) is a scoring system that has been introduced to help clinicians to make decisions in such situations. However, this scoring system has not been shown to be a good predictor of limb amputation or salvage in clinical situations. Thus this remains a challenge when a surgeon is confronted with such a situation. For a surgeon working in isolation in a hospital with limited resources and staff, the challenge becomes even more critical as he/she has to make quick decisions to amputate or perform limb salvage and he may have to perform the function of many specialists. That was the situation I faced on many occasions in the days gone by.
Issues – Surgical, Ethical and Moral Dilemma
Many issues had to be considered when making the decision: Salvage or Amputate
- Danger to the life of the patient as a result of the injury and bleeding
- The extent of the injury
- Whether informed consent can be obtained to perform an amputation in a seriously injured patient in shock/presence or absence of relations to obtain consent etc.
- Anticipated general and local complications if the victim survives.
- Cultural values of the patient
- Whether the limb will be a useless limb or functional with an artificial limb.
- Desire to die rather than suffer an amputation in some societies.
Such views had to be accepted and accommodated in decision making.
Battlefront Injuries of Limbs and Decision Making
While engaged in the battlefront treating battle casualties during the conflict in Sri Lanka there were many occasions where I was confronted with such decision making. In all instances, I had to make rapid decisions. The hospitals where the war victims were treated were settings with limited resources and staff. The surgical team comprised of only one surgeon, one or two house officers supported by an anaesthetist and the nursing staff. There were also limitations concerning the availability of blood, an essential requirement when treating major injuries where there was a severe loss of blood.
The following dictum was followed in managing all the victims with limb injuries. I would have lost the battle concerning limb salvage on occasions, but won the battle with regard to SAVING LIFE and that is what matters finally.
Dear Reader, you might also be interested in my next story, were I would have lost the battle concerning limb salvage on occasions, but won the battle with regard to SAVING LIFE : ‘INAUGURATION OF THE CLINICAL SOCIETY OF POLONNARUWA’

0 thoughts on “The Surgeon’s Dilemma and a Patient’s Worst Nightmare”
Excellent. Remember meeting you for the first time in Polonnaruwa. Then I was a young Major doing Chief Instructor in ITC Minnariya. After that you spoke to me over the radio from Palali in Jul 1991. I was in Eliphent Pass with my Batallion. You gave very clear instructions to me and my AMP late Maj Godamune, ( then he was a WO2) to do an amputation. We saved four lives. Remember good words used by Gen Kobbakaduwa when I explained it to him.
I read this article with rather a confused mind. How did he managed to do this task? And how is he able to gather his thoughts , memories and pen down this traumatic experience?
Certainly a very informative presentation on a surgeon’s dilemma. After all the intention is noble,while the task is rather traumatic. I hope many would be enlightened on this as I am. A must read for all medical students and other laymen.
AMS
Avishka
Thank you. This is surgical decision making at a time of crisis and working with limited resources. The surgeon’s decision must be timely and in the interest of saving the life of the patient even at the expense of losing a limb. Delay may mean death with a limb in tact, recovery is living without a limb. But this can be compensated with an artificial limb, although life may not be the same.
Best wishes
Gamini Goonetilleke
Your experience in this aspect of surgery is immense .I admire your dedication & skills to treat these patients from the battle field . My limited experience in Traumatic amputations is from industrial & road accidents . I totally agree with what you have written, it not only affects the individual but also affects the family . The psychological impact to the patient cold be overwhelming. The long drawn out rehabilitation process could be demanding with the limited resources in SL compared to the West . Well done Gamini & your Rehab. Team
Gamini, another inspiring story of care and healing. You’ve attended to so many catastrophic injuries and operated under such challenging conditions. God bless you always for the care you have shown for suffering humanity.