Treating War Victims Part 3-Antipersonnel Mines

Personal Experiences in the warfront in Sri Lanka
Part 3 -Antipersonnel Mines : “The Devil’s Seed”
Those who hunger for power try “wading through slaughter to a throne” (Alexander Pope)
Antipersonnel landmines are small explosive devices placed underground or fixed above ground and are specifically targeted towards people. These mines come in many different shapes. Often they are camouflaged to blend them into the surroundings and can be fabricated from wood, plastic or metal. They are difficult to locate or detect and are designed to be exploded by the presence, proximity or contact of a person. Antipersonnel mines are usually detonated when they are stepped on or when a tripwire is touched. These mines are designed to incapacitate, injure or kill one or more people. Used mostly in guerilla warfare, antipersonnel mines also serve as a psychological deterrent to advancing combatants.
Commentators on war have described antipersonnel mines as
- The Devil’s seed
- The scourge of modern non-conventional warfare
- One of the most serious man-made problems of our time
- Mines – a perverse use of technology
- The greatest violators of international humanitarian law, practicing blind terrorism
History, Background and Some Country Related Data
The first use of antipersonnel mines dates back to the Second World War when German and Allied troops used them to prevent enemy soldiers from removing anti-tank mines. In the 1960’s the United States (US) introduced a new class of antipersonnel mine, scattered from air and known as remotely delivered mines or “scatterbabies” to stop the flow of men and material from North to South Vietnam through Laos. When stepped on, the device, weighing only 20 gm, could tear off a foot.

This man made epidemic went largely unreported until early 1988, when relief workers drew attention to the large number of limbless victims from mines in Afghanistan and Cambodia. As of today there are at least sixty six (66) States and areas contaminated by antipersonnel mines and 26 States contaminated by cluster ammunition causing injury and death to many combatants and civilians. (Landmine and cluster ammunition monitor)
- The small antipersonnel mines disable those who traverse their paths. The injury potential of this weapon system is primarily focused on the lower extremities, with a fair proportion of those wounded having injuries other than the legs. The high amputation rate of these injuries poses a psychological problem as well as orthopaedic and rehabilitative ones.
- Antipersonnel mines lie dormant until a person activates its firing mechanism. They are blind weapons that cannot distinguish the foot fall of a combatant from that of a non combatant. They recognize no ceasefire and could go on killing and injuring people long after hostilities have ended.
My Experiences

My first exposure to antipersonnel mine injury was at the Base Hospital, Polonnaruwa in 1987. The terrorists had started mining the areas bordering the conflict zones inhabited by civilians. The victim was a young farmer who had gone to his field unaware of the presence of such devices and stepped on a mine. His foot was “blown off” and was admitted to the hospital with severe bleeding. The only treatment I could offer him was an amputation of his leg below the knee joint. He was disabled for life and could not continue his occupation as a farmer anymore with drastic consequences for his family.
With times large swathes of land in strategic areas had been mined by the terrorists to prevent the advancement of troops to the enemy territory. They used both conventional and improvised mines. Initially, the Armed Forces personnel too were unaware of the deployment of mines by the terrorists in these areas. Their advancement resulted in many casualties. Since then many areas in the North- East and the areas bordering this region had been mined by both parties to the conflict. While the majority of the injured were combatants, non combatants including children were also admitted with serious injuries.
CAUTION: SOME PHOTOS THAT FOLLOW MAY NOT BE SUITABLE FOR THE WEAK AND FAINT- HEARTED
“Cries of the Victims”
Soldiers on foot who had stepped on antipersonnel mines had their feet blown off. They were admitted to hospital with heavy bleeding and crying in pain. Some had their foot completely blown off or hanging by a piece of skin or bone. I remember their cries even today. It was indeed a pathetic site to see the wounded with injuries I had never seen before.

They were unemployed village boys who had joined the armed forces to bring some money home and thought that it was the end of their life if they lose the limb. “Sir, please do not cut off my leg, I am the breadwinner of my family, without my leg there is no purpose in living”. For me these pleas were heart-breaking and agonizing! I would never “cut off” a limb if I could save it. At the same time I had to save the life of the victim first. I remembered the dictum which I had learnt during my days as a medical student “save life before limb”. This is a basic principle in surgery which has to be practiced by every surgeon when treating such injuries. Hence amputation of the limb was the procedure that had to be done to save life.
Heart breaking and agonizing pleas of victims – Sir, please don’t cut off my leg
Mines Used
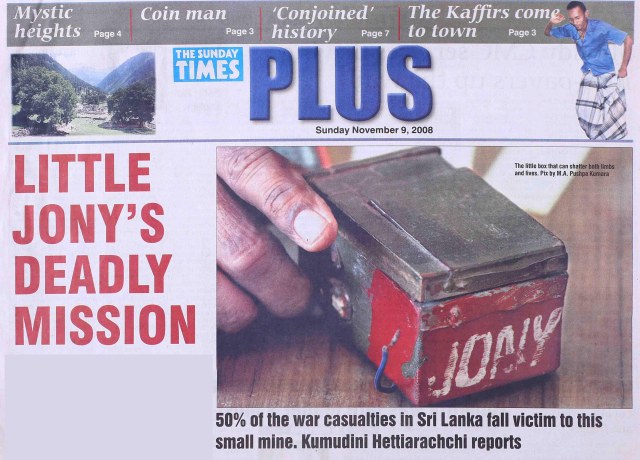
Since 1988 the terrorists had been producing their own antipersonnel mines in jungle hideouts. These were called the “Jony 95” named after a terrorist killed by the Indian Peace Keeping Forces. The cost of producing such a mine was estimated at around Rupees Three Hundred (Rs 300/=). The components of “Jony 95” included a block of wood 11cm x 7cm x6cm, 50g explosive, two pen torch batteries, a detonator, a rubber band, a strip of metal and electric wire.


In 1999 the terrorist produced a modified version of the Jony which was more sophisticated. This was called the Jony 99 or Rangan 99.

Types of Antipersonnel Mines used
- Blast Mine- injury is mainly due to blast effect
- Fragmentation Mines – injury mainly due to fragments or shrapnel dispersed from the mine following detonation.
This is How the Victims were Injured by AP Mines
Pattern 1
The victim activated a mine by stepping on the device. They had a traumatic amputation of part of the foot or the entire foot and sometimes the entire lower limb above the ankle was blown off with less severe injuries elsewhere. Mud, grass, fragments of mine and pieces from the boot were blown upwards into the injured leg, genitals and the buttocks. These injuries were the most severe as there was close contact between the device and the foot when it exploded.
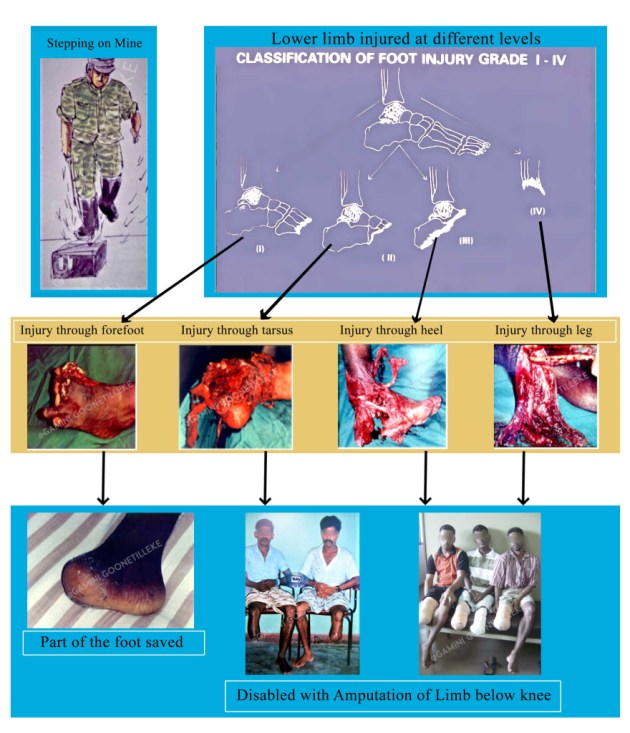
Most of the victims who stepped on mines had an amputation of their lower limb below the knee joint leading to permanent disability.
An Aspect Concerning the Military Boot

A normal military boot does not in any way give protection against an AP mine injury. To mitigate this problem Anti-Mine boots were tried out. These boots were made with an armour- plated sole. The soldiers found it difficult to march with these boots as they were very heavy. Furthermore, in view of the armour-plate the blast effect was deflected even further up leading to injury going above the knee. These were given upas a result.
Pattern 2

The pattern of wounding was more random and consisted of multiple shrapnel wounds from a mine triggered near the victim.
Pattern 3
This injury was common in de-miners trying to locate buried AP mines without protective gear. The mines exploded while being handled resulting in injury to the hands and face and sometimes chest and abdomen. The eyes were damaged by the blast as well as from metallic fragments, mud and sand thrown up by the explosion. Many victims lost their vision in one or both eyes.

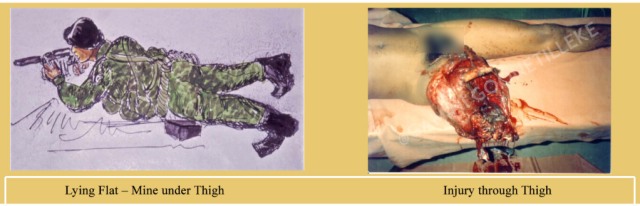
Pattern 4
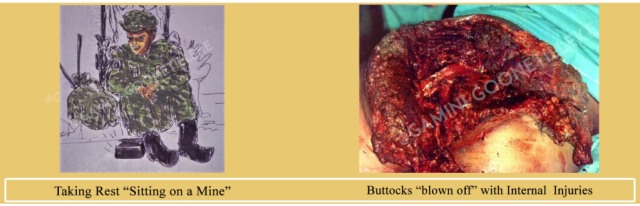
There were occasions when the soldiers had to lie down flat to avoid enemy fire or aim at the enemy. This sometimes happened in mine laden ground resulting in disastrous consequences with injuries affecting various parts of the body such as the lower limb being ripped off. They had an amputation above the knee joint making rehabilitation more difficult. There were also occasions when the soldier would take some rest beneath a tree not knowing that these areas too were mined. The result was a serious injury to the buttocks with damage to internal organs as well.
Management of AP Mine injuries
The management of the victim of an antipersonnel mine should begin at the site of injury with first aid. However, there were severe drawbacks in this aspect during the initial period of war. With time, more and more victims had first aid by field surgical teams. Good first aid meant the difference between life and death. A good pressure dressing that was advocated helped to control bleeding till they reached hospital for further care.

The basic steps include the following-
First aid
- Arrest bleeding with pressure dressing and elevation of the limb
- Splint injured limb
- Resuscitate with intravenous fluids
- Relieve pain
- Start antibiotics – the best antibiotic is Crystalline Penicillin given in a dose of 5 million units intravenously
- Tetanus prophylaxis
Treatment in hospital
- First aid if not given at the site of injury
- Assessment of wounds / extent of injury
- Radiological assessment – to determine the extent of bony damage and identify any radio-opaque foreign bodies. Some of the foreign bodies may not be radio-opaque
- Surgical treatment – wound excision / amputation
Surgery
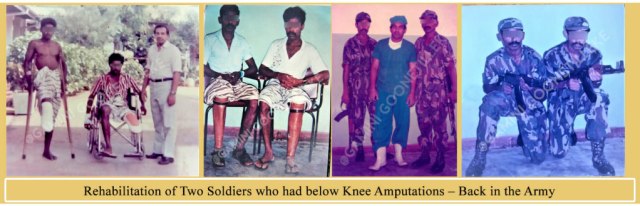
The majority of victims with AP mine injuries to the lower limb required an amputation of the injured limb below the knee joint (80%). The surgical procedure was carried out in order to facilitate the use of an artificial limb so that the victim can be rehabilitated to get back to society and lead a productive life as soon as possible.

Rehabilitation
The victims of antipersonnel mines are disabled for life. The majority are disabled as a result of traumatic amputation of the lower limb, while a smaller number suffer disability as a result of traumatic amputation of the hand, loss of vision or other injuries. Rehabilitation of victims of mine explosions should begin as early as possible. This should include physical exercise to the uninvolved muscles and joints and more importantly psychological rehabilitation. Victims of mines suffer tremendous psychological trauma and may take years to regain confidence. Therefore, this aspect of psychological rehabilitation should not be neglected in the overall management of these victims of land mines.

Continued landmine use is expensive both in stark financial terms and widespread human suffering even during war. The cost is enormous. Therefore, these indiscriminate weapons of war should be should be prohibited















THIS POST IS ONLY ABOUT THE INJURIES CAUSED BY ANTIPERSONNEL MINES DURING THE CONFLICT BASED ON MY PERSONAL EXPERIENCE IN MANAGING THESE INJURIES IN THE WAR FRONT. POST CONFLICT ISSUES CAUSED BY ANTIPERSONNEL MINES AND SOME DATA CONCERNING SRI LANKA WILL BE PUBLISHED IN THE POSTS TO FOLLOW.
Dear Reader, You might want to read the next story more focused on the land mine injuries : ‘ANTIPERSONNEL MINES IN SRI LANKA’

0 thoughts on “Treating War Victims Part 3-Antipersonnel Mines”
Very interesting work you have done, gruesome to look at, thank goodness it is over.
Awesome. God in our midst when observing your works of restoration and healing.
Thank you again for sharing your experiences as a surgeon. As I mentioned before, I am also a general surgeon practicing in a rural area. Although only 40 kms from the city, a lot of patients do not have the financial resources to be admitted in private hospitals. There are 2 tertiary government hospitals in the city but because of the pandemic, there are often on lockdown. Thus, the Iloilo Provincial Hospital where I work he often the hospital of last recourse for patients. Some come from as far as capiz which is more than 100 kms away. I know I will learn a lot from you. Again, my sincerest thanks.