Saving Lives in a Setting With Limited Resources

Three Patients with Injury to Liver
The Liver is a vital organ of the human body. It is very vascular and injury to the liver is associated with bleeding, which sometimes can be fatal. The extent of the injury may vary depending on the causative factor.

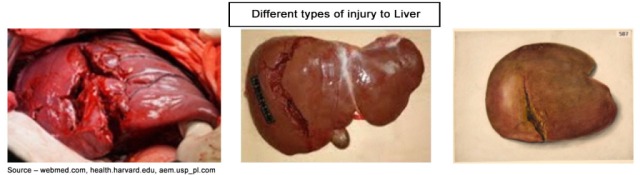
Liver injury may follow both open and closed trauma. Examples of open injury include those caused by a stab which does not produce much damage or a gunshot which can tear and disrupt the liver substance. Closed injuries are those caused by crush injuries as in a road traffic accident with excessive pressure on the right lower chest. It may also be the result of a fall. There may not be any evidence of external injury.
The effects on the patient vary according to the amount of blood loss and bile leakage. There will be a history of injury and signs of blood loss. Some may be admitted in shock due to severe haemorrhage. Examination of the abdomen will also reveal signs of blood inside the abdomen.
Ideally these patients are managed in Specialised Trauma Centres where facilities for specialised investigations such as ultra sound scan, CT scans and other specialised investigations as well as Trauma Teams are available.
The essential immediate care includes resuscitation with blood transfusion to replace the blood lost into the abdominal cavity. The patient should be monitored carefully. If there is no improvement emergency surgery is required to arrest the bleeding and remove damaged areas of the liver followed by repair of the damage by suture. On some occasions the surgeon will have to take a decision to use gauze packs to apply pressure on the damaged area of the liver to stop the bleeding from the liver. Subsequently the abdomen has to be reopened to remove the gauze packs. This can be a life saving procedure and is called “Damage Control Surgery”
As I have mentioned earlier, Polonnaruwa Hospital where I worked in the 1980’s was a Rural Hospital with limited resources and I was the only surgeon there to treat all types of injuries. I recollect having performed surgery on three patients who were admitted to the hospital with extensive injury to the liver way back in 1985. I had to manage these patients with whatever resources that was available to save their lives. I did not consider transferring these patients to “Big” hospitals for obvious reasons. The closest hospitals in the chain of transfer were situated in Matale / Kandy more than 100 km away. This would have taken have taken over 4 hours on bumpy roads and death would have been inevitable due to bleeding from the ruptured liver.
Case 1
This was a Policeman who was shot by an unknown gunman with a shotgun. This happened in the early hours of the morning while he was on security duty close to a Police station in a remote area. The bullet hit him on his belly. He suffered serious injury and collapsed to the ground. On hearing the noise of firing his fellow Policemen rushed to the scene, found him collapsed, carried him into a Police jeep and dispatched him to the Polonnaruwa Hospital 30 km away. As usual he did not have any first aid or an ambulance to transport him to hospital. On arrival at the hospital, I was called into see the patient. He was in a state of shock and collapse. The entry wound of the gunshot was in the right upper abdomen with the exit wound on the right flank. The bullet exiting the body was followed by the protrusion of the small intestine through the exit wound. There was no doubt that he needed emergency surgery after resuscitation with intravenous fluid and blood. I proceeded to open his belly, an operation called Laparotomy to arrest the bleeding inside the abdomen not knowing from where he was bleeding into the abdominal cavity.

What did I find at Surgery and what was done?
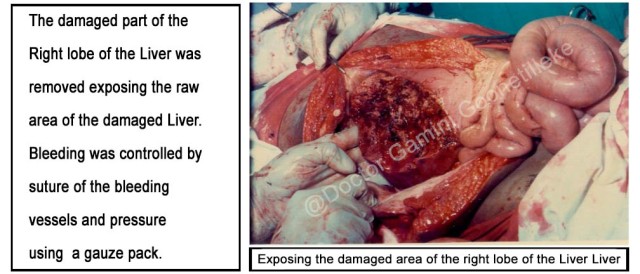
It was obvious that the bowel protruding out could not have caused bleeding and shock. In view of the site of the injury the most likely organ to have been injured and caused bleeding would have been the Liver. As I opened the abdomen blood poured out of the abdominal cavity. The blood inside the abdominal cavity was sucked out to inspect the Liver. I noticed extensive damage to the right lobe of the Liver. The bowel that had come out had to be withdrawn into the cavity before assessing the actual damage to the Liver. As there was extensive damage to that part of the Liver it had to be removed leaving a raw area in the Liver with areas of bleeding. The bleeding vessels had to be sutured and further oozing of blood was controlled by pressure with a gauze pack. There was no damage to the bowel or any other organ. The bowel was replaced in its normal position. Blood transfusion was carried out during and after the operation to replace the blood lost. The patient required in all 10 pints of blood. He recovered without any postoperative complications.




KEY POINTS IN MANAGING A RUPTURED LIVER
- Early admission to hospital – although in those reported in this article, there was considerable delay due to lack of transport.
- Rapid assessment and resuscitation with intravenous fluid and blood transfusion
- Emergency surgery without delay
- Remove damaged parts of the liver / suture
- If bleeding cannot be controlled – Damage Control Surgery. Control bleeding with guaze packs. Remove packs at a second operation once the patient’s condition is stabilised.
- A Surgeon available on the spot to perform emergency surgery.
- Practicing these key points will help to save life in settings with limited resources, I hope !
Dear Reader, You might be interested to read my next post as well : ‘HONOUR PHYSICIANS FOR THEIR SERVICES, FOR THE LORD CREATED THEM’ and the other following post were I share about highway robbers / criminals who terrorized the area in 1980s : ‘HIGHWAY ROBBERS IN POLONNARUWA IN THE 1980’S AND A FUNERAL BY THE ROADSIDE’

0 thoughts on “Saving Lives in a Setting With Limited Resources”
This is great
Your contribution and service to this country and the people should never be forgotten
What you have done and achieved is so remarkable and no greater blessing than saving lives !
You are an instrument of healing in God’s hand
God bless your hands that heal.