Shot in the Belly, Bowel’s out
Admitted to Hospital 12 hours Later
Before the on set of the war in the North-East of the country, gunshot victim admissions were few at the Polonnaruwa Hospital. They were mostly victim so flow-velocity (less than 300 m/s) fire arms such as shotguns.
Occasionally, a surgeon may encounter unusual problems like what I experienced at the Base Hospital, Polonnaruwa. This is a story of a 30 year-old man who was shot-at and faced numerous issues before recovering and going home.
He was on his way home with a few friends when he was shot. The bullet had hit him on the left side of the belly. He had collapsed to the ground and his stomach, small intestine and large intestine had come out instantaneously. In medical terms this is “evisceration”.He was at least 70 Km from the hospital and no one present could find an ambulance or any other vehicle to take him to the closest hospital, the Base Hospital in Polonnaruwa where I was the only surgeon.
While awaiting some form of transport, he had informed his friends who were with him that he felt thirsty and hungry. His friends had no idea of first aid and there were no paramedics to attend to him.The friends gave-in to the injured friend’s request and fed him well with a combination of king coconut water, rotti, dhal and meat curry. The patient was happy, but not for long. His condition aggravated in that the stomach that was out of the belly ballooned out and he was in sheer distress. His friends were panicking, unable to find a vehicle to take him to hospital. In the mean time the patient’s condition deteriorated.Finally, when he reached the hospital, lying on the floor of a van, 12 hours had elapsed.
On admission to my ward he was in a critical condition and in a state of shock. He was pale, with a low blood pressure, a weak but rapid pulse and breathing rapidly indicating shock and in imminent danger of losing his life. In addition, the stomach that had ballooned out was tense and could have ruptured any moment. This was a serious condition that I had never seen before or read in any text book or medical journal.
That was on a Sunday afternoon around 3 PM on a day where the only anesthetist in the hospital was on leave.My first duty was to resuscitate him before thinking of anything else. That was by infusion of intravenous fluid and blood.
After that I had to take an even difficult decision within a very short period of time. What could I do without an anaesthetist? One way out was to transfer him to another hospital but that was 140 Km away. However, I knew that if I set about to transfer him he could have died on the way. Hence,without any hesitation I accepted the challenge and took the bold decision to treat him even though there was no anaesthetist in the hospital. I discussed the condition with my supporting staff and they all agreed with my decision.
Stages of the procedure to save life:
After resuscitation, the patient was wheeled into the operating theatre. Without anaesthesia a small nick was made in the ballooned out stomach and 1½ litres of fluid together with food residue was drained out. The stomach collapsed immediately. The nick was stitched.
The next step needed anaesthesia. I induced anaesthesia with a Thipentone injection,relaxed his abdominal muscles with another injection of a muscle relaxant (Scoline). A tube called the endotracheal tube was inserted into his trachea to ventilate him after connecting it to the Anaesthetic machine. I requested my House Officer to observe his vitals as there were no monitors to do so. Yes, you read it right; there were no monitors whatsoever!
With the relaxation of the abdominal muscles the stomach that was now collapsed was pushed into the abdominal cavity through the opening created by the gunshot. Next I examined the small bowel that was out. That was not damaged and therefore it was pushed in.
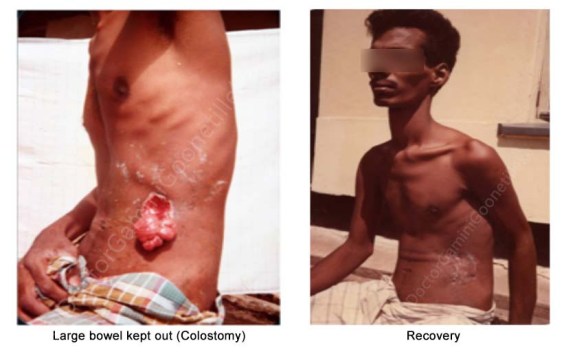
Another issue was seen at this stage. The large bowel that had come out was damaged. In such a situation the safest procedure is to leave that part of the bowel out. This is described as a colostomy. That was the end of the emergency surgery and the patient was weaned away from the anaesthetic machine which was supporting his breathing. On recovery he was taken to the general ward. There was no Intensive care Unit and that care was given in the ward by my dedicated staff under my supervision.
With further treatment he gradually improved and recovered completely. Later on that part of the large bowel that was kept out was repaired with success. The entire procedure was carried out through the same “hole” made by the unknown gunman as shown in the photograph.

Working under conditions with limited facilities and resources, I had to use my discretion in this life-threatening situation. It was a risk, but risks had to be taken in the interest of the patient with the sole aim of saving his precious life. I had to go the extra mile and beyond my specialty carrying out the dual role of surgeon and anaesthetist. These adventurous procedures,are rarely required today.
A challenge awaits us surgeons with the dawn of each new day. It is there for the asking and it is up to us to decide to take-up the challenge or not. If we act positively, besides helping the unfortunate victims we will be richer from that experience.
Dear Reader, you might be interested to read my next post, A boy who was shot through his head : ‘SURVIVES GUNSHOT INJURY THROUGH HEAD!’
Please feel free to share story this with your friends :
6 thoughts on “Shot in the Belly, Bowel’s out”
The work of human hands
Very rare to hear these days.Amazing!!!
Bravo doctor. Well done. When the going gets tough, the tough gets going. No high end technology or modern equipment. Just common sense and the will to save a life.
Roy- Thank you. I like your comment very much. Common sense and the will to save a life are the key words Doctors should always have in their mind. Keep reading my Blog. Best wishes. Gamini Goonetilleke
Another interesting read. The photos remind me of Japanese men who had committed hara kiri.
In the cause of service to the Nation